
Reassessing Nanoparticle Immunotoxicity: From Well-Established To Novel Approaches
By Marina A. Dobrovolskaia, Nanotechnology Characterization Lab., Cancer Research Technology Program, Frederick National Laboratory for Cancer Research

Nanotechnology offers unprecedented capabilities to many biomedical applications, including targeted drug delivery, vaccines, gene- and immune-therapies, tissue engineering, imaging agents, image-guided surgery, medical devices, and diagnostics.1-4 However, translating these complex products from the bench to the clinic is impeded by several barriers: logistical (e.g., funds availability and access to Good Manufacturing Practice facilities), scientific (e.g., understanding complex nano-biointeractions and overcoming limitations of current in vitro and in vivo models), technological (e.g., scale-up manufacturing), societal (e.g., acceptance or refusal of a new technology by people), and political (e.g., rigidity of established regulatory frameworks for drug approval).5 Some promising nanomedicines, despite demonstrating safety in early clinical trials, have failed to cross the so-called translational “valley of death” due to logistical reasons, while others failed the rigor of safety testing, with immunotoxicity being a common culprit, leading not only to clinical trial failures but also to the withdrawal of approved drugs during the post-marketing stage.6
The Double-Edged Sword Of Nanoparticles-Immune System Interactions
The interaction between nanoparticles and the immune system is a double-edged sword. On one hand, these interactions can be purposefully harnessed for therapeutic benefits, as seen with lipid nanoparticle-based mRNA vaccines and immunotherapies. On the other hand, unintended immune recognition frequently leads to adverse events compromising safety, rapid clearance compromising efficacy, and prolonged retention in the body, which can compromise both long-term safety and efficacy. Over the past two decades, the scientific community has developed a robust understanding of many nanoparticle-immune interactions.7,8 Well-known sources of adverse immune-mediated responses to nanomedicines, such as hemolysis, complement activation, perturbation of normal blood coagulation (due to interactions with platelets and coagulation factors), and activation of mononuclear cells producing cytokines, have been extensively investigated. Importantly, these investigations have enabled the connection of specific nanoparticle physicochemical properties (e.g., size, zeta potential, composition, surface functionalities, and hydrophobicity) to these toxicities.8,9 This knowledge has formed the current foundation for establishing nanomedicines’ critical quality attributes and has informed the regulatory framework for their review and approval.
However, as nanomedicine evolves, new challenges emerge, demanding a re-evaluation of our assessment paradigms. Despite these successes, interactions between nanoparticles and specific subsets of immune cells (e.g., mast cells, basophils, and neutrophils), and the molecular mechanisms underlying these interactions, remain incompletely understood or are entirely neglected in traditional preclinical testing.10 Furthermore, the precise intracellular fate of nanoparticles and the consequences of their distribution within subcellular compartments are often overlooked. Collectively, these limitations highlight the urgent need for new models and approaches.
Herein, I highlight government-funded resources available to the extramural community to de-risk nanomedicines, review foundational principles of immunotoxicity testing, and discuss emerging models and methodologies that improve our understanding of nanoparticles’ immunotoxicity.
The NCL Assay Cascade: A Foundational Resource for Nanomedicine Developers
To help the research community navigate preclinical challenges and assist in crossing the translational "valley of death," the U.S. government established a critical infrastructure supporting the preclinical development of nanomedicines. Central to this mission is the Nanotechnology Characterization Laboratory (NCL), established by the National Cancer Institute in collaboration with the National Institute of Standards and Technology and the U.S. FDA. The NCL serves as a resource dedicated to advancing nanomedicine by providing the extramural research community with comprehensive, standardized, and rigorous characterization of nanoparticle therapeutics via its Assay Cascade program (Figure 1).
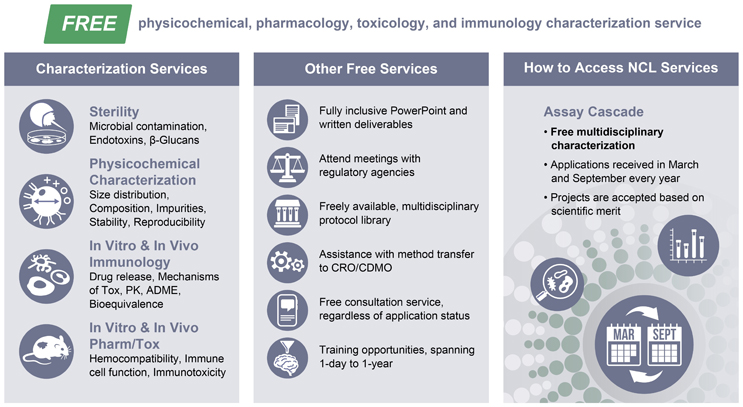
Figure 1. Nanotechnology Characterization Laboratory (NCL) Assay Cascade Program. The NCL’s assay cascade includes standardized methods for analysis of nanomaterials’ sterility and contamination with innate immune response-modulating impurities, physicochemical characterization, and in vitro and in vivo immunology, pharmacology, and toxicology. These services and other services shown on the above image are provided to the extramural research cancer nanomedicine community free of charge for the submitting investigator.
Cancer nanomedicine developers can submit their concepts for characterization in the standardized assay cascade encompassing physicochemical, pharmacological, toxicological, and immunological characterization (here). The NCL’s assay cascade includes standardized methods for analysis of nanomaterials’ sterility and contamination with innate immune response-modulating impurities, physicochemical characterization, and in vitro and in vivo immunology, pharmacology, and toxicology. These services and other resources shown in Figure 1 are provided to the extramural cancer nanomedicine community free of charge. Applications for the NCL Assay Cascade characterization services are accepted based on scientific merit twice a year. The application process is available here.
Established Models For Immunotoxicity Assessment
Immunotoxicity encompasses a variety of adverse effects on the immune system, including suppression, enhancement, and modulation of normal immune responses. These effects can be desired, such as in the case of immunosuppressive drugs used to prevent organ transplant rejection, or adverse, such as the unintended immunosuppression caused by cytotoxic oncology drugs. Adverse immunosuppression and immunostimulation are associated with recurrent infections and hypersensitivity reactions, respectively. Immunomodulation is a peculiar type of immunotoxicity not associated with overt enhancement or suppression, but rather changes the way the immune system responds to otherwise suppressive or stimulatory substances. Established preclinical models and analytical frameworks are well suited to screen immunosuppressive and immunostimulatory substances but may require modifications to adequately screen for immunomodulation.
For nanomedicines, immunotoxicity may result from the nanocarrier, the active pharmaceutical ingredient (API), or both; it may also originate from excipients added to formulations. It is equally important to both identify immunotoxicity and understand its source early in development. The established immunotoxicity framework for nanomedicines capitalizes on the current knowledge of immunotoxicity testing of different drug types (small molecules, therapeutic nucleic acids, and biologics) and is presented in Figure 2 below. This staged approach begins with screening for innate immune response-modulating impurities, such as endotoxin and beta-glucans, which may compromise immunology safety and efficacy studies.
In vitro hematology assays (hemolysis, platelet aggregation, plasma coagulation, and complement activation) are then used to assess the nanomaterial’s compatibility with blood, while in vitro immune cell function assays (cytokine secretion, phagocytosis, leukocyte proliferation, human lymphocyte activation [HuLa], etc.) assess effects on white blood cell function.
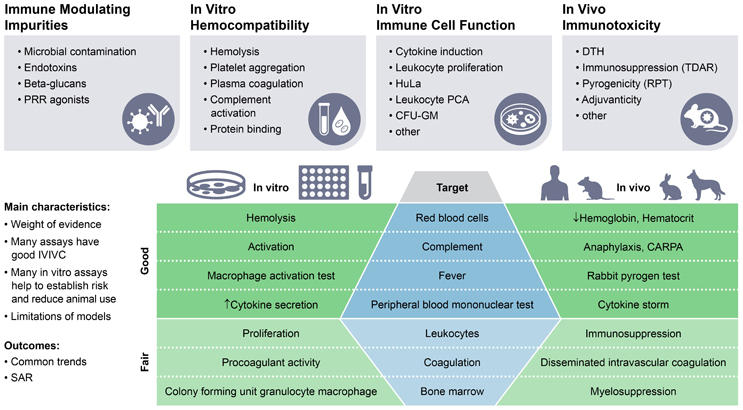
Figure 2. Preclinical Immunotoxicity Framework. This framework was established in the Nanotechnology Characterization Laboratory (NCL) in the early 2000s and validated across various types of nanomaterials, including over 600 nanoparticle-based lead formulations that passed through the NCL Assay Cascade Program. Full-length protocols are available to the public here.
PRR – pattern recognition receptors; PCA – procoagulant activity;
CFU-GM – colony forming unit granulocyte macrophage; DTH – delayed type hypersensitivity;
TDAR – T-cell dependent antibody response; RPT – rabbit pyrogen test;
IVIVC – in vitro in vivo correlation; SAR = structure-activity relationship;
CARPA – complement activation related pseudoallergy.
Many of these in vitro tests have an established record of in vitro-in vivo correlation (IVIVC).11 For example, in vitro assays for complement activation and cytokine secretion are widely recognized for their ability to predict the risk of complement activation-mediated pseudoallergy (CARPA) syndrome and cytokine storm, respectively.12-15 According to the recent FDA guidance for industry, when such in vitro assays establish a risk of immunotoxicity, an in vivo study for the same toxicity is not required.16
Finally, specialized in vivo immune function tests (e.g., T-cell-dependent antibody response [TDAR] for immunosuppression and colony-forming unit granulocyte-macrophage (CFU-GM) assay for myelosuppression) are used to assess specific types of immunotoxicity based on the evidence from general toxicity studies or in vitro assays that require follow-up. While in vitro assays can help decrease animal use in establishing immunotoxicity risks, they cannot completely replace animal studies. For example, a positive in vitro colony forming unit–granulocyte/macrophage (CFU-GM) assay result indicating toxicity to hematopoietic stem cells still needs in vivo verification, as the in vitro finding becomes irrelevant if the nanoparticles do not distribute to the bone marrow in vivo. Unlike small molecules, formulation of the same drug on different nanoparticle platforms results in a drug product with different drug release kinetics and different biodistribution, which collectively may dramatically change both the drug’s safety and toxicity profiles, thus making in vivo models irreplaceable for nanomedicine.
Common acute immunotoxicities of nanotechnology-based carriers include hemolysis, alterations in platelet function (aggregation or alteration of the aggregation caused by a known agonist), plasma coagulation times, complement activation, cytokine secretion, and alterations in the activated lymphocyte function or hematopoietic stem cell differentiation. Examples demonstrating a connection between nanocarrier-mediated responses and physicochemical properties are summarized in Figure 3 below and have been discussed in detail elsewhere.8,9
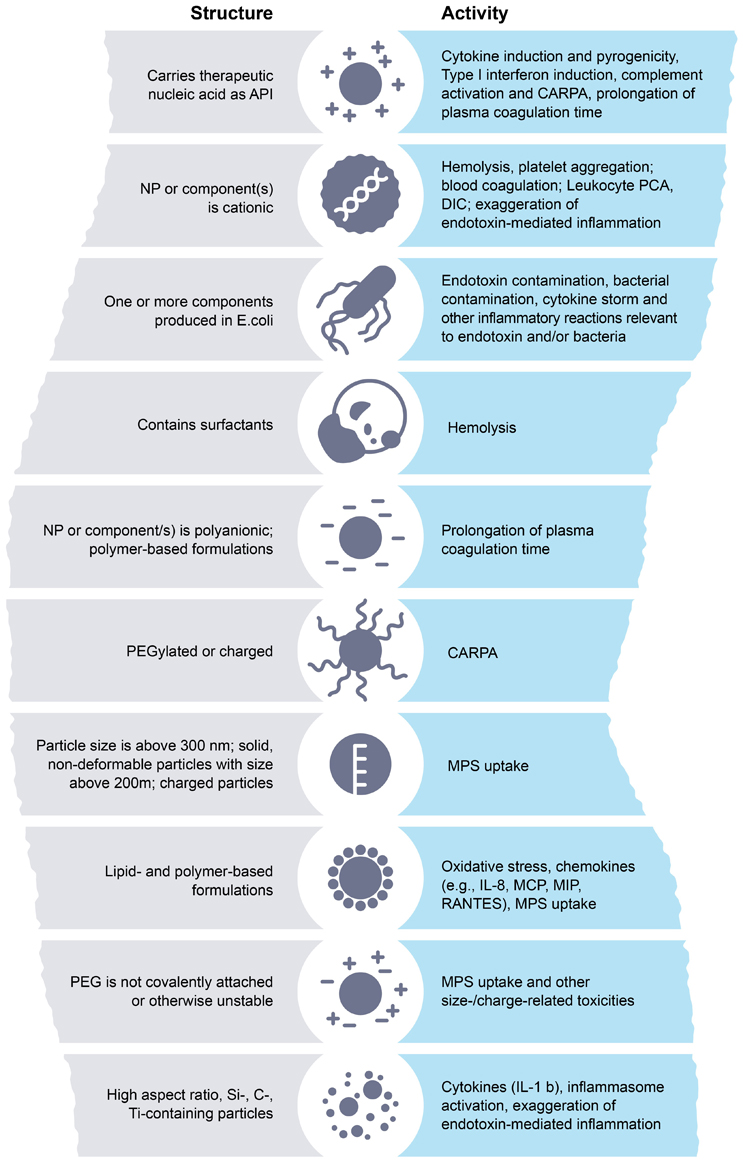
Figure 3. Structure-Activity Relationships (SARs) in Nanoparticle-Mediated Immunotoxicity. Common acute immune-mediated responses are summarized. Nanoparticle physicochemical properties are shown in boxes on the left. Their corresponding immunological responses are on the right. While many factors, including dose and route of administration, also play a key role in immunotoxicity, knowing these SARs helps to prioritize preclinical studies and limited resources to first test for and address the highly likely immunotoxicities before running more resource-intensive full-scale general toxicity studies.
API – active pharmaceutical ingredient; PCA – procoagulant activity;
DIC – disseminated intravascular coagulation; CARPA – complement activation related pseudoallergy;
MPS – mononuclear phagocytic system; NP – nanoparticles; IL-interleukin;
MCP – monocyte chemoattractant protein; MIP – macrophage inflammatory protein;
RANTES – Regulated on Activation Normal T Expressed and Secreted.
These structure–activity relationships (SARs) are invaluable. By understanding these SARs, researchers can prioritize preclinical studies and allocate limited resources effectively to test for and address highly likely immunotoxicities before more resource-intensive full-scale general toxicity studies. This proactive approach helps establish the weight-of-evidence for immunotoxicity, validate in vitro methods, understand their IVIVC, and reasonably reduce the use of research animals, all while reliably establishing immunotoxicity risk. Furthermore, this approach provides insight into common trends in immunocompatibility across various nanotechnology drug delivery platforms (e.g., platelet aggregation, hemolysis, exaggeration of endotoxin-mediated inflammation by cationic carriers, and prolongation of plasma coagulation times by hydrophilic, long, polar, charged polymeric carriers).8,9
Despite these successes, the current approach has limitations. Established and validated in vitro or in vivo models are not yet available for all clinically relevant immunotoxicities, challenging their identification during the preclinical stage. Mechanisms underlying some immune-mediated adverse effects are also incompletely understood, challenging the process of developing relevant methods and models to screen for these toxicities. Furthermore, the precise interactions between nanocarriers and specific immune cell subsets, including their effector functions and their underlying mechanistic relationships, the intracellular fate of nanoparticles, and their distribution within subcellular compartments, remain incompletely understood. Collectively, these limitations drive the urgent need for new models.
New Approaches: Addressing Emerging Challenges and Unmet Needs
New approaches and models are being developed to overcome the known limitations of traditional models, enabling a preclinical immunotoxicity framework to catch toxicity early and more accurately. These alternatives also aim to refine methodologies, reduce animal use, and accelerate preclinical testing. Toxicities poorly predicted by existing preclinical models, or those showing significant deviations from human patient responses, are usually primary targets for such novel methodologies.
For example, hand-and-foot syndrome or palmar-plantar erythrodysesthesia (PPE) is a common immune-mediated skin toxicity associated with cancer chemotherapy drugs. Due to its complexity, animal models notoriously fail to accurately replicate PPE, highlighting an urgent need for alternative models. The skin explant co-culture model (Skimune) is one such example that bridges this gap. This assay, initially developed by Anne Dickinson at Newcastle University, involves co-culturing human skin biopsies with autologous peripheral blood mononuclear cells (PBMCs) or monocyte-derived dendritic cells. It analyzes biomarkers of inflammation and skin damage and has shown effectiveness in identifying biologics and small molecules with a risk of inducing immune-mediated reactions such as skin sensitization, cytokine storm, Graft-versus-Host Disease, and immunogenicity.17-19 Recently, this assay showed good in vitro-clinical correlation for PPE induced by PEGylated liposomal doxorubicin (Doxil) and free doxorubicin.20 Of note, applying the skin explant assay to nanomaterial screening required a modification of the reporting structure to account for the drug release from the nanocarrier and different effects of the drug and the nanocarrier on the assay components. While validation of this assay for other nanomedicines is still needed, the initial results with Doxil and doxorubicin are very encouraging.
The research community is also making significant strides in leveraging machine learning (ML) and artificial intelligence (AI) to predict immunotoxicity, which heavily relies on high-quality experimental data. For example, SAR data generated by testing a comprehensive library of nucleic acid nanoparticles (NANPs) in human PBMCs enabled the development of quantitative SAR models and an AI algorithm for predicting NANP-mediated interferon responses based on particle composition and physicochemical properties.21-23 Currently, this model is limited to NANPs delivered using lipid-based carriers. As more extensive SAR data accumulate, expansion of the current model to include NANP-mediated cytokine responses across other delivery carriers becomes increasingly feasible.
Unraveling Intracellular Immunotoxicity:
Beyond predictive modeling and improved in vitro systems for known toxicities, a critical area of emerging research lies in understanding immunotoxicities that originate inside cells, an area largely neglected by traditional immunotoxicity assays. For example, while the complement system is widely known for its cascade activation in blood plasma, leading to acute reactions like CARPA,13,14 research now indicates that complement proteins are also found intracellularly within immune cells.24,25 Moreover, the intracellular complement system (ICS) represents a non-canonical immune pathway with distinct characteristics from its plasma counterpart. Specifically, plasma complement is activated outside the cell, typically leading to acute toxicity through binding of split products (anaphylatoxins) to cell surface receptors and triggering immune cell activation; the adverse effects of plasma complement activation can often be mitigated by simply removing the activating agent. In contrast, intracellular complement activation occurs inside the cell and may lead to more insidious, chronic toxicity or contribute to autoimmune-like conditions; as such, removing the external nanoparticle may not resolve the ongoing intracellular activation. Importantly, the link between ICS, chronic inflammation, and autoimmunity has not yet been established, urgently calling for more research in this area.
Initial studies with nanoparticles reveal fascinating SARs for ICS activation.26 Interestingly, nanoparticles known to cause severe hypersensitivity reactions or activate plasma complement (e.g., Doxil, Taxol) do not appear to activate the ICS.26 Instead, the primary activators of ICS appear to be nanoparticles that affect the integrity of cellular membranes. Specifically, cationic nanoparticles have been identified as potent ICS activators.26 Further work with cationic dendrimers has elucidated key physicochemical determinants. Specifically, zeta potential plays a key role, as amine-terminated (cationic) particles are strong ICS activators, whereas neutral or anionic counterparts show minimal activity.26 Size and surface functional group density are important, as larger particles and those with a higher density of surface amine groups exhibit significantly increased reactivity.26 The particle architecture, beyond just charge, also plays a critical role, as demonstrated by differences in responses to cationic poly(amidoamine) (PAMAM) versus triazine dendrimers, pointing to the role of the density and presentation of reactive groups on the particle surface.26
This new understanding has profound implications for drug delivery. Cationic nanoparticles are widely employed for the delivery of nucleic acids (siRNA, mRNA, plasmid DNA), where intracellular delivery is paramount. This research suggests a previously overlooked safety liability that may potentially contribute to chronic, low-grade inflammation or autoimmune-like conditions, which would entirely bypass detection by standard complement assays assessing the function of the plasma complement. While an in vitro assay, ITA-26, developed at the NCL helps screen nanoparticles to assess ICS activation,27,28 more research is needed to fully understand both the biology of ICS and its relevance to nanomedicine safety. Moreover, as was previously noted, the specificity of commercial antibodies used in ICS research is a critical factor that not only may affect the accuracy of mechanistic studies but also create a significant hurdle in assay reproducibility and data interpretation.26
Conclusion and Future Outlook
While preclinical immunotoxicity is well managed by traditional frameworks and models, and well supported by government-funded resources like the NCL's Assay Cascade, the future of nanomedicine safety lies in expanding these traditional frameworks to enable reliable and faster screening for immunotoxicities that the traditional methodology fails to accurately and timely detect. Thinking beyond standard tests, we need to consider the full nanoparticle life cycle, including its interactions with cells, internalization, and intracellular fate, and fully understand the mechanisms of nanoparticle interactions with various subsets of immune cells. A better understanding of molecular mechanisms (e.g., intracellular complement activation) and effects on neglected immune cells (e.g., mast cells, basophils, and neutrophils) is crucial for future studies.
By implementing cutting-edge technologies to understand complete transcriptomic, proteomic, and interactomic changes at a single-cell level, and leveraging advanced models to get mechanistic insights, one can build a more complete safety profile covering all potential nanoparticle–immune cell interactions and link each adverse immune-mediated response to nanoparticle physicochemical properties. Such a nuanced and comprehensive understanding of nano-immune interactions will enable a more efficient design of safer and more effective nanomedicines, ultimately accelerating their translation from bench to bedside. A consortium joining efforts between government, industry, and academia would be instrumental in realizing this vision. Well-established, government-funded infrastructures like the NCL can be vital in catalyzing such joint efforts.
This project was funded by federal funds from the National Cancer Institute, National Institutes of Health, under contract 75N91019D00024. The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the U.S. Government
References
- Mullick, P., andManna, A., 2025.Nano-biomaterials: Emerging tools in biomedical innovation and therapy. Current Opinion in Biomedical Engineering 36, 100627.
- Huang, X.,Kong, N.,Zhang, X.,Cao, Y.,Langer, R., andTao, W., 2022.The landscape of mRNA nanomedicine. Nat Med 28, 2273–2287.
- Kirtane, A. R.,Verma, M.,Karandikar, P.,Furin, J.,Langer, R., andTraverso, G., 2021.Nanotechnology approaches for global infectious diseases. Nat Nanotechnol 16, 369–384.
- Gomerdinger, V. F.,Nabar, N., andHammond, P. T., 2025.Advancing engineering design strategies for targeted cancer nanomedicine. Nat Rev Cancer 25, 657–683.
- Dobrovolskaia, M. A., 2026.When small gets smart: how the application of nanotechnology is transforming immunology in the 21(st) Century. Nanomedicine (Lond) 21, 1097–1115.
- 2025.Q&A Translational Cancer Nanomedicine. Nature Communications 16, 8288.
- Crist, R. M.,Barenholz, Y.,Cern, A.,Clark, K. N.,Cullis, P. R.,Dean, C.,Desai, N.,Ferrari, M.,Germain, M.,Giacomantonio, C. A.,Grabarnik, E.,Grodzinski, P.,Hod, A.,Kennedy, B. E.,Kularatne, R. N.,Kwon, G. S.,Loeb, E.,Noftall, E. B.,Pagliaro, L.,Rasoulianboroujeni, M.,Roth, A.,Rowles, D.,Singh, K.,Steinmetz, N. F.,Yehtina, Z.,Zhang, Y.,Zilbersheid, D.,Clogston, J. D.,Stern, S. T., andDobrovolskaia, M. A., 2025.Advancing Medical Applications of Cancer Nanotechnology: Highlighting Two Decades of the NCI'S Nanotechnology Characterization Laboratory Service to the Research Community. Wiley Interdiscip Rev Nanomed Nanobiotechnol 17, e70020.
- Dobrovolskaia, M. A., 2025.Charting new frontiers in nanoparticle immunotoxicity: A perspective on current, emerging, and future approaches. Biochem Biophys Res Commun 777, 152280.
- Dobrovolskaia, M. A., 2022.Lessons learned from immunological characterization of nanomaterials at the Nanotechnology Characterization Laboratory. Front Immunol 13, 984252.
- González-Fernández, Á., andMaietta, I., 2025.The Forgotten Innate Immune Cells: Unraveling Their Prospective Interactions with Nanomaterials. Int J Nanomedicine 20, 8173–8189.
- Dobrovolskaia, M. A., andMcNeil, S. E., 2013.Understanding the correlation between in vitro and in vivo immunotoxicity tests for nanomedicines. J Control Release 172, 456–66.
- Bedőcs, P., andSzebeni, J., 2020.The Critical Choice of Animal Models in Nanomedicine Safety Assessment: A Lesson Learned From Hemoglobin-Based Oxygen Carriers. Front Immunol 11, 584966.
- Szebeni, J., 2018.Mechanism of nanoparticle-induced hypersensitivity in pigs: complement or not complement? Drug Discov Today 23, 487–492.
- Szebeni, J., andBawa, R., 2020.Human Clinical Relevance of the Porcine Model of Pseudoallergic Infusion Reactions. Biomedicines 8.
- Dobrovolskaia, M. A., andAfonin, K. A., 2020.Use of human peripheral blood mononuclear cells to define immunological properties of nucleic acid nanoparticles. Nat Protoc 15, 3678–3698.
- US FDA, Nonclinical Evaluation of the Immunotoxic Potential of Pharmaceuticals. HHS, Ed. Center for Drug Evaluation and Research: 2023; Vol. FDA-2019-D-5607.
- Ahmed, S. S.,Ahmed, M. M.,Ishaq, A.,Freer, M.,Stebbings, R., andDickinson, A. M., 2024.An In Vitro Human Skin Test for Predicting Skin Sensitization and Adverse Immune Reactions to Biologics. Toxics 12.
- Martins-Ribeiro, A.,Kizhedath, A.,Ahmed, S. S.,Glassey, J.,Ishaq, A.,Freer, M., andDickinson, A. M., 2024.A Human Skin Explant Test as a Novel In Vitro Assay for the Detection of Skin Sensitization to Aggregated Monoclonal Antibodies. Toxics 12, 332.
- Ahmed, S., andDickinson, A., 2021.Detecting immunotoxicity in vitro—clinically relevant studies in the COVID-19 era. Journal of Pharmacological and Toxicological Methods 111, 107000.
- Cedrone, E.,Ishaq, A.,Grabarnik, E.,Edmondson, E.,Skoczen, S.,Neun, B. W.,Freer, M.,Shuttleworth, S.,Sviland, L.,Dickinson, A., andDobrovolskaia, M. A., 2024.In vitro assessment of nanomedicines' propensity to cause palmar-plantar erythrodysesthesia: A Doxil vs. doxorubicin case study. Nanomedicine 62, 102780..
- Johnson, M. B.,Halman, J. R.,Satterwhite, E.,Zakharov, A. V.,Bui, M. N.,Benkato, K.,Goldsworthy, V.,Kim, T.,Hong, E.,Dobrovolskaia, M. A.,Khisamutdinov, E. F.,Marriott, I., andAfonin, K. A., 2017.Programmable Nucleic Acid Based Polygons with Controlled Neuroimmunomodulatory Properties for Predictive QSAR Modeling. Small 13.
- Johnson, M. B.,Jain, S.,McMillan Shea, J.,Krueger, Q.,Doe, E.,Miller, D.,Pranger, K.,Hayth, H.,Thornburgh, S.,Halman, J.,Khisamutdinov, E. F.,Zakharov, A. V., andAfonin, K. A., 2025.From Sequence to Response: AI-Guided Prediction of Nucleic Acid Nanoparticles Immune Recognitions. Small 21, e09459.
- Chandler, M.,Jain, S.,Halman, J.,Hong, E.,Dobrovolskaia, M. A.,Zakharov, A. V., andAfonin, K. A., 2022.Artificial Immune Cell, AI-cell, a New Tool to Predict Interferon Production by Peripheral Blood Monocytes in Response to Nucleic Acid Nanoparticles. Small 18, e2204941.
- Afzali, B.,Singh, P.,Tajmul, M., andKemper, C., 2025.Inside job: Roles of intracellular C3. J Allergy Clin Immunol 156, 215–223.
- West, E. E.,Afzali, B., andKemper, C., 2018.Unexpected Roles for Intracellular Complement in the Regulation of Th1 Responses. Adv Immunol 138, 35–70.
- Ilinskaya, A. N.,Shah, A.,Enciso, A. E.,Chan, K. C.,Kaczmarczyk, J. A.,Blonder, J.,Simanek, E. E., andDobrovolskaia, M. A., 2019.Nanoparticle physicochemical properties determine the activation of intracellular complement. Nanomedicine 17, 266–275.
- Ilinskaya, A.,Shah, A.,Van Dusen, A., andDobrovolskaia, M. A., 2024.Detection of Intracellular Complement Activation by Nanoparticles in Human T Lymphocytes. Methods Mol Biol 2789, 109–120.
- Ilinskaya, A. N.,Shah, A., andDobrovolskaia, M. A., Detection of Intracellular Complement Activation in Human T Lymphocytes: Version 1. In National Cancer Institute’s Nanotechnology Characterization Laboratory Assay Cascade Protocols, National Cancer Institute (US): Bethesda (MD), 2005.
Competing Interests
The author has no interests to disclose.
About The Author:
 Marina A. Dobrovolskaia, Ph.D., MBA, PMP is the Laboratory Co-Director, Director of Operations, and the Head of the Immunology Section at the Nanotechnology Characterization Laboratory (NCL). In her role as the head of the Immunology Section, Dobrovolskaia leads a team that conducts preclinical studies to monitor nanoparticles’ toxicity to the immune system, in vitro and in vivo, using the standardized NCL Assay Cascade. Before joining the NCL in 2005 to establish the immunology Assay Cascade, Dobrovolskaia worked as a research scientist in a GLP laboratory at PPD Development, Inc. in Richmond, VA, where she was responsible for designing, developing, and validating bioanalytical ligand-binding assays to support pharmacokinetic and toxicity studies in various drug development projects, and completed postdoctoral trainings at the National Cancer Institute and the University of Maryland. She has published over 200 manuscripts, which generated over 23,000 citations (h-index 63). She can be reached at marina@mail.nih.gov.
Marina A. Dobrovolskaia, Ph.D., MBA, PMP is the Laboratory Co-Director, Director of Operations, and the Head of the Immunology Section at the Nanotechnology Characterization Laboratory (NCL). In her role as the head of the Immunology Section, Dobrovolskaia leads a team that conducts preclinical studies to monitor nanoparticles’ toxicity to the immune system, in vitro and in vivo, using the standardized NCL Assay Cascade. Before joining the NCL in 2005 to establish the immunology Assay Cascade, Dobrovolskaia worked as a research scientist in a GLP laboratory at PPD Development, Inc. in Richmond, VA, where she was responsible for designing, developing, and validating bioanalytical ligand-binding assays to support pharmacokinetic and toxicity studies in various drug development projects, and completed postdoctoral trainings at the National Cancer Institute and the University of Maryland. She has published over 200 manuscripts, which generated over 23,000 citations (h-index 63). She can be reached at marina@mail.nih.gov.